-
Digestive system and its diseases or pachan tantra ane tena rogo
Author: Dr Sanjiv Haribhakti
Publisher: Kaizen Hospital
Published: 2011Digestive system and its diseases or pachan tantra ane tena rogoRead More -
The SAGES Manual fundamentals of laparoscopy,thoracoscopy and GI endoscopy second edition
Author: Carol E H Scott - Conner
Publisher: Springer
Published: 2006The Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) ManualRead More -
 Author: Dr V K Kapoor
Author: Dr V K Kapoor
Publisher: Shubham Book Distributors, Lucknow, India
Published: 2010Tips for safe cholecystectomyRead More- Adequate formal training in minimal invasive surgery, preferably during
- post graduation or alternatively as an observer but not merely by attending workshops over weekends
- Proper selection of initial cases - thin built female patient with short history of biliary colics only, no history of acute cholecystitis, thin walled distended gall bladder on ultrasound
- Proper informed consent (including chances of conversion and higher risk of bile duct injury)
- Good quality equipment and instruments
- Proper cleaning and sterilisation of instruments
- A qualified and trained surgeon as the first assistant
- Urinary bladder evacuated just before anaesthesia and surgery
- General anaesthesia
- Open insertion of first canula
- 30° telescope
- All instruments must be introduced, operated and removed under vision
- Fundus retracted upwards towards right shoulder
- Gall bladder neck retracted down and out
- Remember that every patient has his/ her own biliary and vascular anatomy in the Calot’s triangle
- Cystic lymph node is an important landmark – keep to its right
- No cautery in Calot’s triangle – it should be used in gall bladder bed only
- Suction canula is a good instrument for blunt dissection
- Hug the gall bladder, not the bile duct
- Clipping of the cystic duct flush with the common bile duct is not required
- It is safer to leave a few mm of cystic duct than to encroach even 1 mm on the common bile duct
- Double clips on the retained side of the cystic duct and cystic artery
- Ligature, Haemoclip, Endoloop and stapler are useful devices to tackle a
- wide cytic duct
- Normal sized common bile duct can easily be mistaken for cystic duct
- Beware of wide cystic duct, long cystic duct, vertical cystic duct – it may
- be common bile duct
- Very soft (normal) liver, fatty liver and cirrhotic liver can easily be injured
- during retraction
- Fundus first is a useful technique in difficult cases
- Partial cholecystectomy is an option in case of difficulty
- Panic should be avoided in case of bleeding
- Pressure with a gauze or the mobilised gall bladder will control the bleeding or make it controllable
- Desperate blinds attempts to clip or coagulate a bleeding point in a pool of blood must be avoided
- Stumps (cystic duct/ cystic artery) should be examined and re-examined for security of clips and any bile leak/ bleed
- Gall bladder bed should be irrigated and examined for any bleed/ bile leak (from a cholecysto-hepatic duct)
- Presence of bile should make the surgeon stop and look for the source of bile - gall bladder or bile duct
- Extraction of gall bladder under vision to make sure that there is no bile/
- stone spill
- Spilled bile should be sucked out
- Spilled stones should be looked for and removed
- Aponeurosis at 10 mm port sites should be closed
- Surgeon should not have any ego to complete every cholecystectomy
- laparoscopically
- Conversion is a safety valve and an emergency exit
- Have a low threshold for conversion
- Conversion is not a failure on the part of the surgeon
- Cholecystectomy should not be considered a small/ routine operation and should not be taken lightly/ casually
- Surgeons should avoid the temptation to get their names into books of
- records
- Experience is no protection against bile duct injury
- All gall bladders, even if they look grossly normal, should be sent for
- histopathology so as not to miss an incidental gall bladder cancer
- The day after cholecystectomy, the patient should be without pain, sitting up in the bed, having her breakfast and wanting to go home – vitals should be stable/ normal and abdomen soft; if not, observe the patient in the hospital for another day
- In the era of increasing medical litigation, a safe cholecystectomy is safe
- not only for the patient but for the surgeon also
-
Blumgart's Surgery of the Liver, Biliary Tract and Pancreas (5th Edition) English
Author: William R. Jarnagin
Publisher: Saunders
Published: 4 May 2012Read MoreThis 2-volume reference, edited by a panel of experts and featuring contributions by many leading authorities, comprehensively covers the cutting edge of research, teaching, and practice in surgery of the liver, biliary tract, and pancreas. This resource covers anatomy, pathophysiology, immunology, molecular biology, genetics, diagnosis, and treatment. At www.expertconsult.com you can not only access the complete contents online, but also an abundance of detailed illustrations and step-by-step procedural video clips from the Memorial Sloan Kettering video library that show you how to perform key procedures step by step.
-
Baily Loves Short Practice of Surgery (I/E) (26th Edition) English
Author: Norman S Williams, Christopher JK Bulstrode, P Ronan O'Connell
Publisher: CRC/T&F
Published: 2013Read MoreThe ISE Edition of one of the world's pre-eminent medical textbooks, beloved by generations of surgeons both in the UK and in numerous countries overseas, with lifetime sales in excess of one million copies.
An essential book that every practising doctor should have leave aside Surgeons. The revised edition is livid with colorful photographs and detailed text. Recommended for any budding surgeon. The additional facts given in the revised edition is of great help to understand the subject well.
| Photos |
|---|
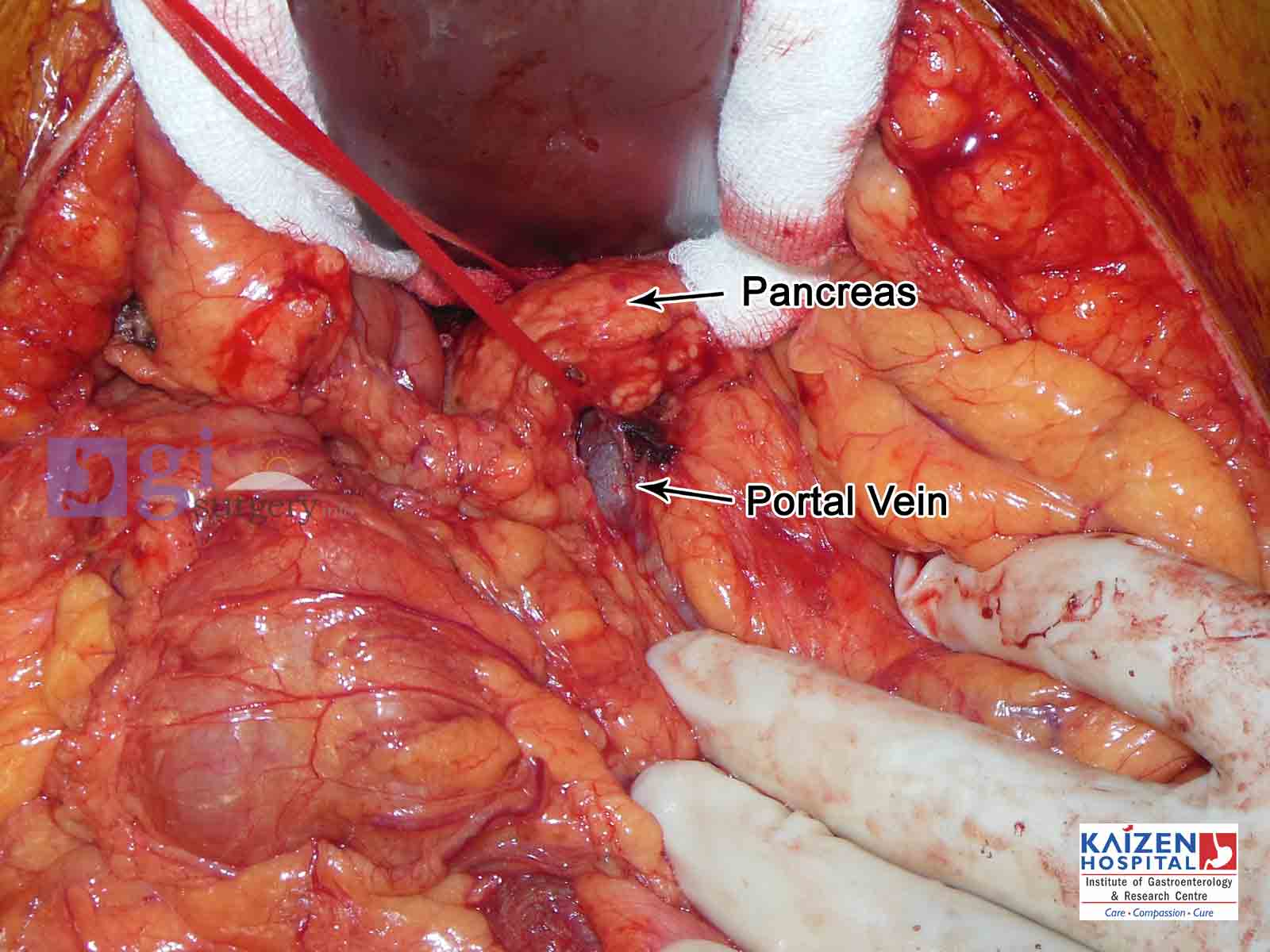
| Whipple's operation |
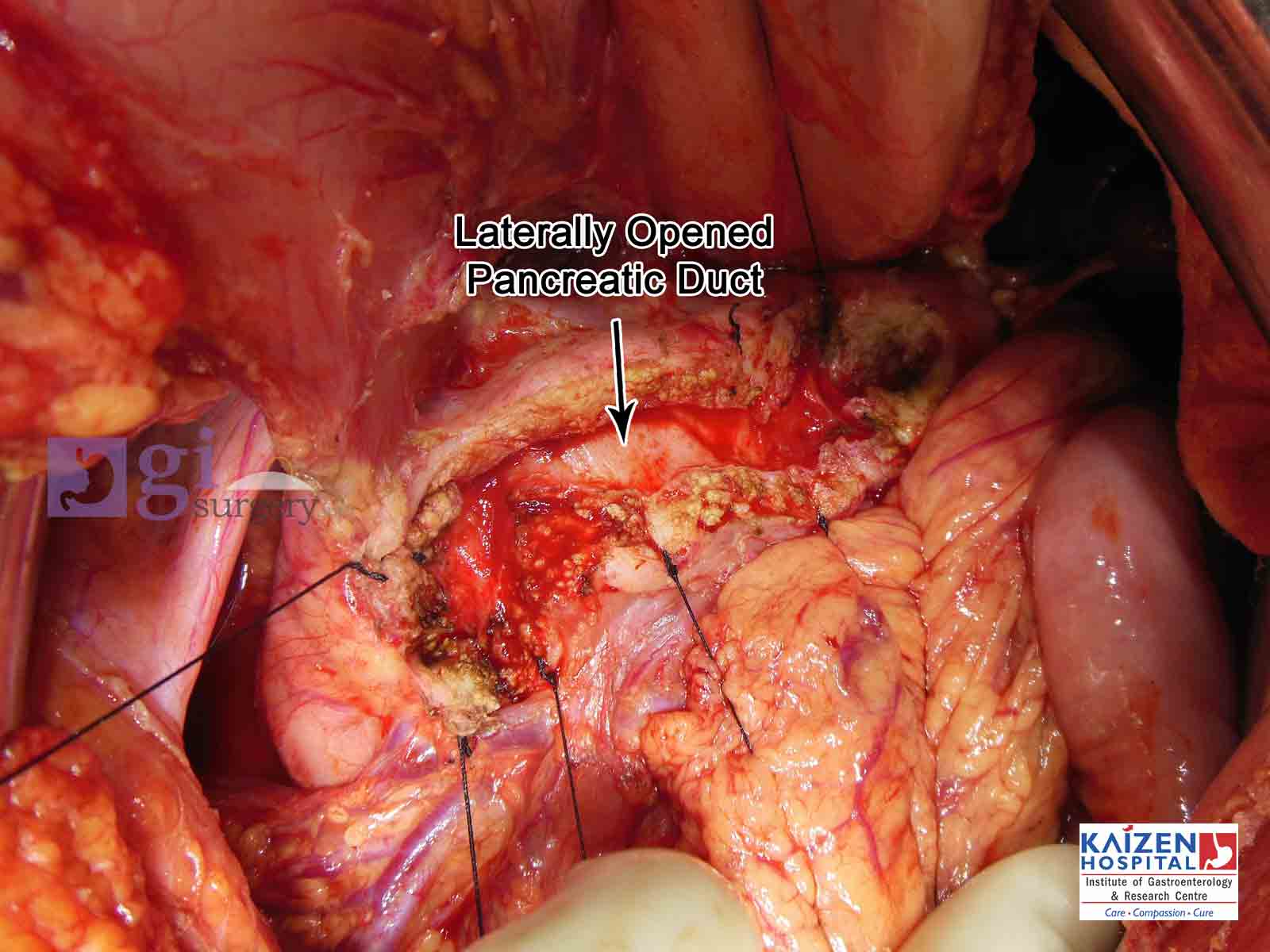
| Opened pancreatic duct |
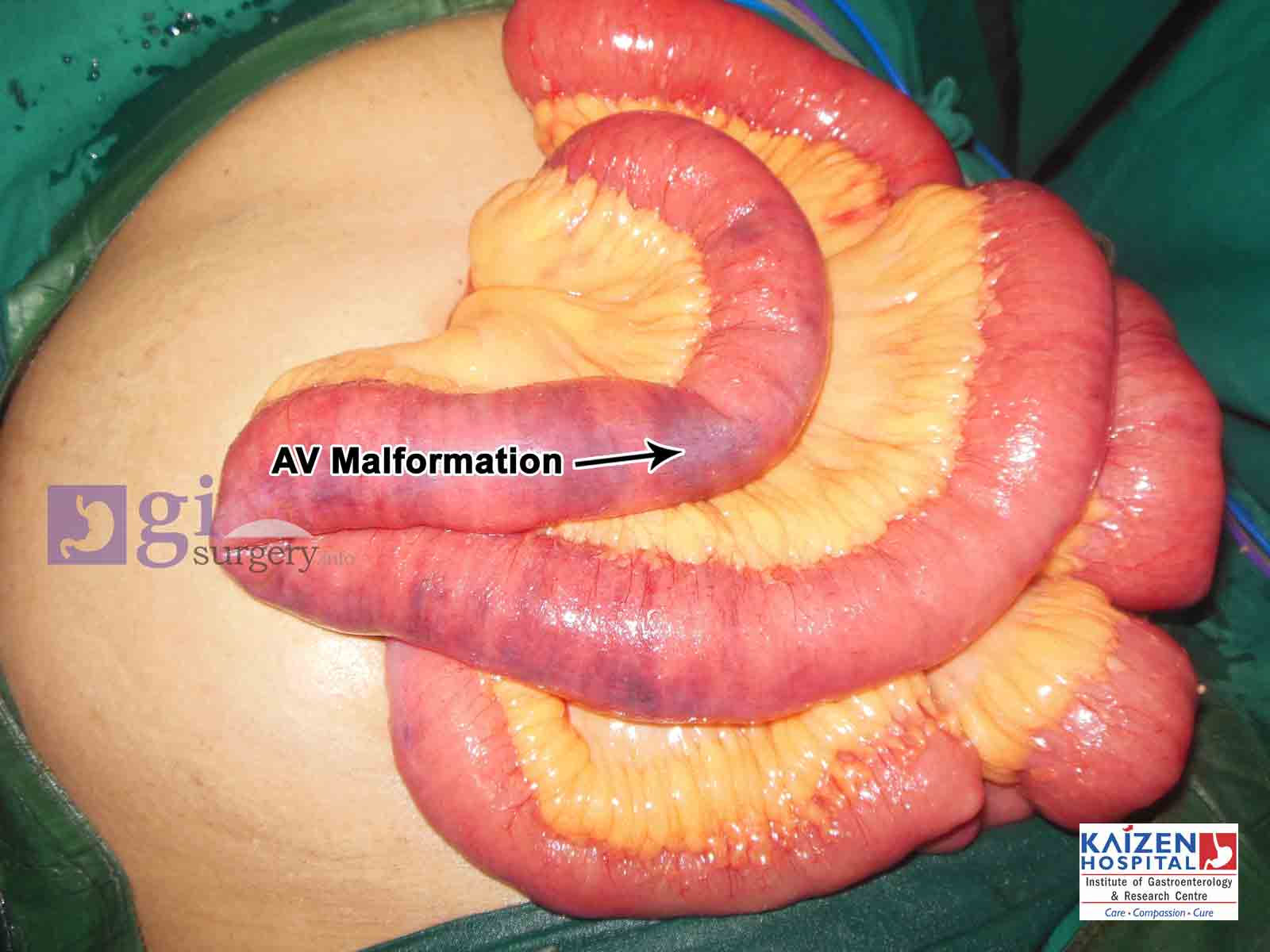
| AV Malformation of small intestine |
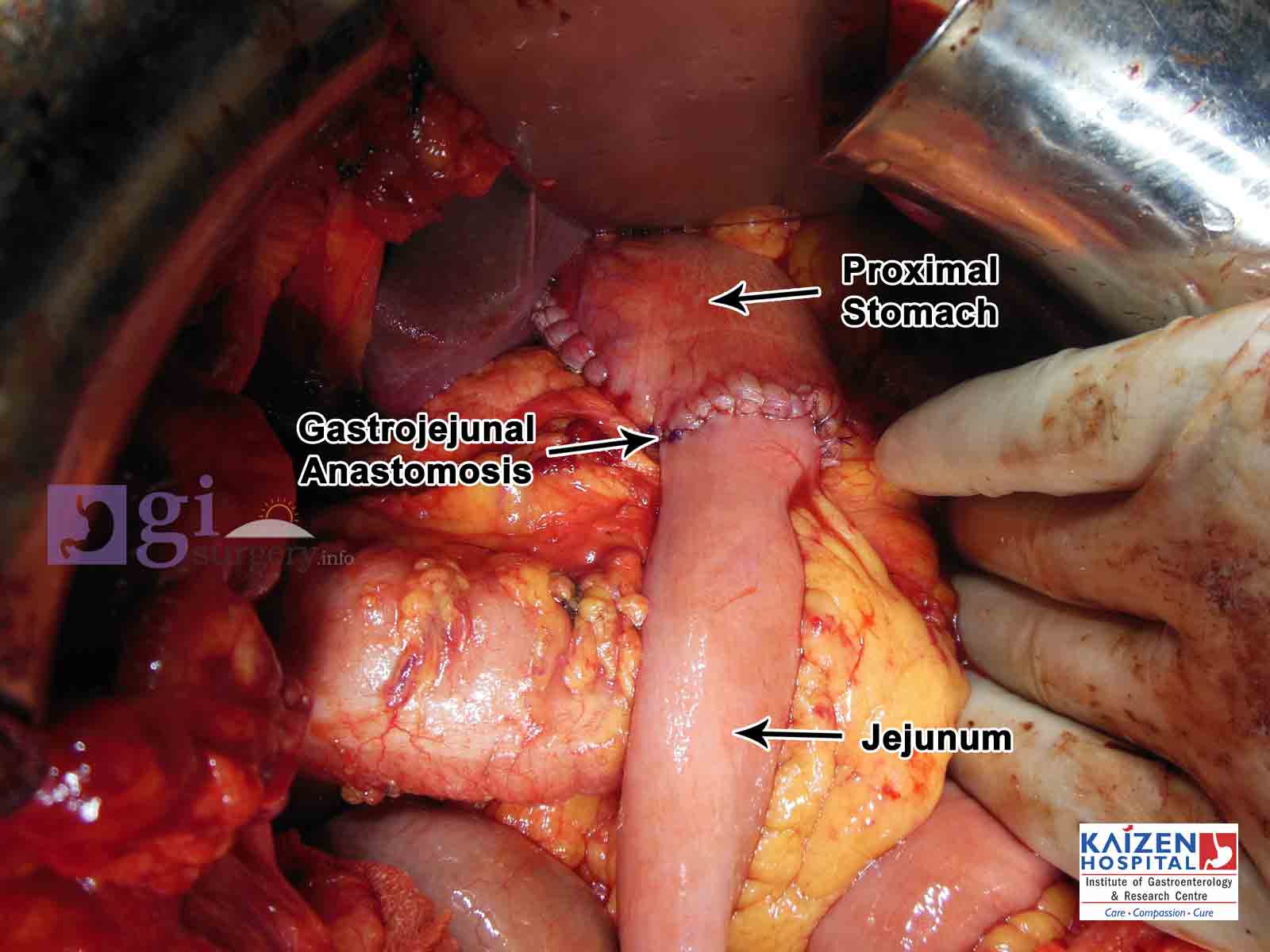
| Ca Stomach and patial gastrectomy |
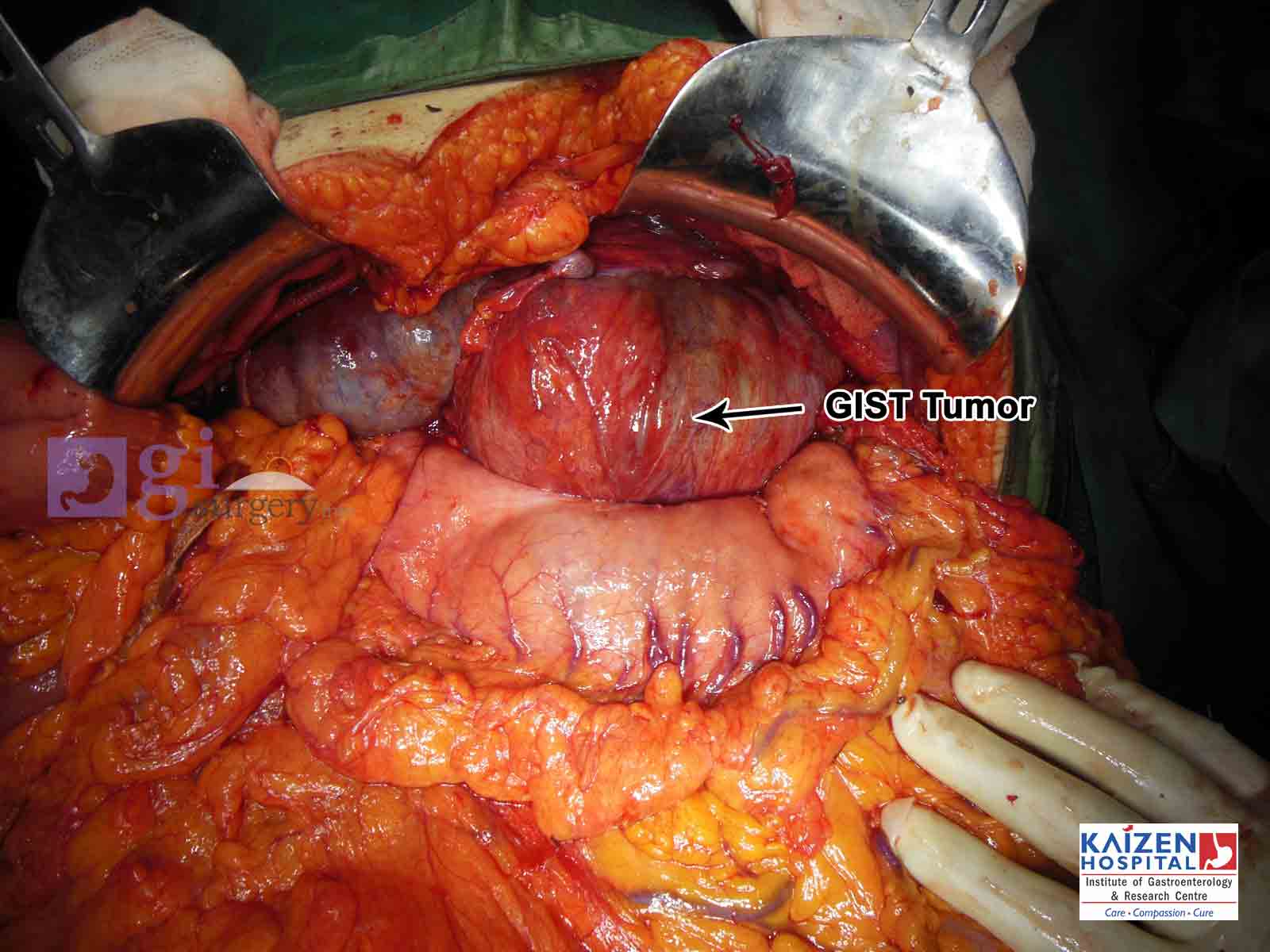
| GIST tumour |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}