Biliary Tract Cancers Show Tumor-Specific Gene Features
by Chase Doyle
San Francisco—Two-thirds of biliary tract cancer patients harbored genomic alterations that could soon guide the selection of approved targeted therapies or access to novel therapies available in clinical trials, according to findings presented at the 2015 Gastrointestinal Cancers Symposium.
“Given the limited treatment options and poor prognosis of patients with biliary tract cancers, and the diversity of clinically relevant alterations that have been identified in this study … comprehensive genomic profiling [has] significant potential to maximize the identification of new treatment paradigms and meet an unmet clinical need for this devastating disease,” said investigator Jeffrey Ross, MD, medical director of Foundation Medicine and chair of the Department of Pathology and Laboratory Medicine at Albany Medical College, in New York.
According to Dr. Ross, biliary tract cancers—including intrahepatic cholangiocarcinoma (IHCCA), extrahepatic cholangiocarcinoma (EHCCA) and gallbladder carcinomas (GBCA)—typically present at an advanced stage and are refractory to conventional cytotoxic chemotherapy. The study’s goal was to determine whether comprehensive genomic profiling of IHCCA, EHCCA and GBCA would reveal distinctive patterns of genomic alterations and identify clinically relevant alterations that could lead to targeted therapies.
The study used a hybrid capture-based next-generation sequencing assay that evaluated the coding exons of 315 cancer-related genes and 47 introns in genes commonly rearranged in cancer. DNA was extracted from 554 biliary tract carcinomas, including 412 cases of IHCCA, 57 cases of EHCCA and 85 cases of GBCA.
The overall number of genomic alterations per patient was similar among the various types of biliary tract carcinomas (Table). The clinically relevant alterations—the so-called “actionable alterations” per patient—also were the same: two for all three tumor types.
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
For patients with IHCCA, “There was a wide diversity in the type of alterations,” Dr. Ross said.TP53 was the most commonly altered gene, followed by P16, KRAS and others. For the GBCA group, TP53 also was the most commonly altered gene. KRAS was the most commonly altered gene for EHCCA, followed by TP53 and P16.
IHCCA, EHCCA and GBCA all were noted to have frequent genomic alterations associated with cell cycle regulation (CDKN2B) and chromatin remodeling (ARID1A). IHCCA was further characterized by FGFR fusions, IDH1/2 substitutions, BRAF substitutions and MET amplification, with a low KRAS mutation frequency. IHCCA and GBCA had frequent ERBB2 amplifications and PI3KCA/MTOR pathway alterations. KRAS mutation frequency was high in EHCCA and low in GBCA.
Dr. Ross noted that amplification of the ERBB2 gene—potentially the same as in breast and upper gastroesophageal carcinomas—was found in 16% of patients with GBCA. The ERBB2amplification rate was lower in patients with EHCCA (11%) and even lower in patients with IHCCA (4%).
Dr. Ross highlighted several cases in which patients responded to targeted therapies in each of the three tumor types. For example, one patient with an EGFR-amplification GBCA responded to neoadjuvant erlotinib (Tarceva, Genentech) therapy when it was combined with systemic chemotherapy. In another case, a GBCA patient with FGFR3 fusion demonstrated disease stability after four months of the investigational agent dovitinib. “This suggests, that targeting the FGFR fusion has clinical efficacy for this tumor type,” Dr. Ross said.
Dr. Ross stressed that the findings were preliminary and were meant to identify potential therapeutic targets. “We did not use this study as a prognostic test; it was only done to search for therapy targets,” he said. “We do not have the kind of outcomes data for the entire cohort to be able to put prognostic results into the study at this point, but we’re hoping to get that kind of follow-up.”
Clinical Trials Needed
Laura A. Dawson, MD, a researcher for the Cancer Clinical Research Unit at the Princess Margaret Cancer Centre, in Toronto, Canada, said, “I think moving forward, we need to change the way we make treatment decisions, and I think this is the way of the future—to look at not only pathological or anatomical histology but profiling as well. [These] results validate some others that have looked at the biliary tract, so it’s very exciting—there’s huge promise here. However, we still need to do this in a clinical trial, because a mutation does not necessarily mean it will benefit with an agent that hits the mutation. So, I strongly believe we need to incorporate profiling into trials.”
Although Dr. Dawson said she would use profiling with her patients, she cautioned that it would be unethical to do so without the proper mechanism to treat the patient, such as a clinical trial.
“And for trials that aren’t using profiling,” she concluded, “I strongly recommend the archiving of tissue—or to look for serum and circulating DNA—so we can learn in a prospective setting whether targeting actual mutations should differ from standard care.”
Payment also is a problem, Dr. Meropol argued. Increasingly, payors are scrutinizing off-label use of expensive targeted agents, resulting in costs falling on patients. “Recommending cancer drugs with high copays may not be ethical without strong evidence that they are going to help that individual patient,” he said. Given the potential for confusion over interpretation, Dr. Meropol stressed the importance of knowing who is interpreting the data and making recommendations. He concluded his talk with a focus on the patients. “We don’t want to give our patients false hope,” he said. “We don’t want to subject them to the risks of needless biopsies, and we don’t want to subject them to the financial burden of therapies and procedures that are not destined to help.”
After both speakers completed their presentations, the audience response shifted somewhat. After the presentations, fewer participants stated that they would routinely order genomic tests than had indicated they would in a baseline survey before the debate. Nevertheless, 60% of the audience polled still said they would recommend an assay for a patient with metastatic colon cancer refractory to treatment if the gene-sequencing panel was covered by insurance.
Biliary Tract Cancers Show Tumor-Specific Gene Features
by Chase Doyle
San Francisco—Two-thirds of biliary tract cancer patients harbored genomic alterations that could soon guide the selection of approved targeted therapies or access to novel therapies available in clinical trials, according to findings presented at the 2015 Gastrointestinal Cancers Symposium.
“Given the limited treatment options and poor prognosis of patients with biliary tract cancers, and the diversity of clinically relevant alterations that have been identified in this study … comprehensive genomic profiling [has] significant potential to maximize the identification of new treatment paradigms and meet an unmet clinical need for this devastating disease,” said investigator Jeffrey Ross, MD, medical director of Foundation Medicine and chair of the Department of Pathology and Laboratory Medicine at Albany Medical College, in New York.
According to Dr. Ross, biliary tract cancers—including intrahepatic cholangiocarcinoma (IHCCA), extrahepatic cholangiocarcinoma (EHCCA) and gallbladder carcinomas (GBCA)—typically present at an advanced stage and are refractory to conventional cytotoxic chemotherapy. The study’s goal was to determine whether comprehensive genomic profiling of IHCCA, EHCCA and GBCA would reveal distinctive patterns of genomic alterations and identify clinically relevant alterations that could lead to targeted therapies.
The study used a hybrid capture-based next-generation sequencing assay that evaluated the coding exons of 315 cancer-related genes and 47 introns in genes commonly rearranged in cancer. DNA was extracted from 554 biliary tract carcinomas, including 412 cases of IHCCA, 57 cases of EHCCA and 85 cases of GBCA.
The overall number of genomic alterations per patient was similar among the various types of biliary tract carcinomas (Table). The clinically relevant alterations—the so-called “actionable alterations” per patient—also were the same: two for all three tumor types.
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
For patients with IHCCA, “There was a wide diversity in the type of alterations,” Dr. Ross said.TP53 was the most commonly altered gene, followed by P16, KRAS and others. For the GBCA group, TP53 also was the most commonly altered gene. KRAS was the most commonly altered gene for EHCCA, followed by TP53 and P16.
IHCCA, EHCCA and GBCA all were noted to have frequent genomic alterations associated with cell cycle regulation (CDKN2B) and chromatin remodeling (ARID1A). IHCCA was further characterized by FGFR fusions, IDH1/2 substitutions, BRAF substitutions and MET amplification, with a low KRAS mutation frequency. IHCCA and GBCA had frequent ERBB2 amplifications and PI3KCA/MTOR pathway alterations. KRAS mutation frequency was high in EHCCA and low in GBCA.
Dr. Ross noted that amplification of the ERBB2 gene—potentially the same as in breast and upper gastroesophageal carcinomas—was found in 16% of patients with GBCA. The ERBB2amplification rate was lower in patients with EHCCA (11%) and even lower in patients with IHCCA (4%).
Dr. Ross highlighted several cases in which patients responded to targeted therapies in each of the three tumor types. For example, one patient with an EGFR-amplification GBCA responded to neoadjuvant erlotinib (Tarceva, Genentech) therapy when it was combined with systemic chemotherapy. In another case, a GBCA patient with FGFR3 fusion demonstrated disease stability after four months of the investigational agent dovitinib. “This suggests, that targeting the FGFR fusion has clinical efficacy for this tumor type,” Dr. Ross said.
Dr. Ross stressed that the findings were preliminary and were meant to identify potential therapeutic targets. “We did not use this study as a prognostic test; it was only done to search for therapy targets,” he said. “We do not have the kind of outcomes data for the entire cohort to be able to put prognostic results into the study at this point, but we’re hoping to get that kind of follow-up.”
Clinical Trials Needed
Laura A. Dawson, MD, a researcher for the Cancer Clinical Research Unit at the Princess Margaret Cancer Centre, in Toronto, Canada, said, “I think moving forward, we need to change the way we make treatment decisions, and I think this is the way of the future—to look at not only pathological or anatomical histology but profiling as well. [These] results validate some others that have looked at the biliary tract, so it’s very exciting—there’s huge promise here. However, we still need to do this in a clinical trial, because a mutation does not necessarily mean it will benefit with an agent that hits the mutation. So, I strongly believe we need to incorporate profiling into trials.”
Although Dr. Dawson said she would use profiling with her patients, she cautioned that it would be unethical to do so without the proper mechanism to treat the patient, such as a clinical trial.
“And for trials that aren’t using profiling,” she concluded, “I strongly recommend the archiving of tissue—or to look for serum and circulating DNA—so we can learn in a prospective setting whether targeting actual mutations should differ from standard care.”
Payment also is a problem, Dr. Meropol argued. Increasingly, payors are scrutinizing off-label use of expensive targeted agents, resulting in costs falling on patients. “Recommending cancer drugs with high copays may not be ethical without strong evidence that they are going to help that individual patient,” he said. Given the potential for confusion over interpretation, Dr. Meropol stressed the importance of knowing who is interpreting the data and making recommendations. He concluded his talk with a focus on the patients. “We don’t want to give our patients false hope,” he said. “We don’t want to subject them to the risks of needless biopsies, and we don’t want to subject them to the financial burden of therapies and procedures that are not destined to help.”
After both speakers completed their presentations, the audience response shifted somewhat. After the presentations, fewer participants stated that they would routinely order genomic tests than had indicated they would in a baseline survey before the debate. Nevertheless, 60% of the audience polled still said they would recommend an assay for a patient with metastatic colon cancer refractory to treatment if the gene-sequencing panel was covered by insurance.
| Photos |
|---|
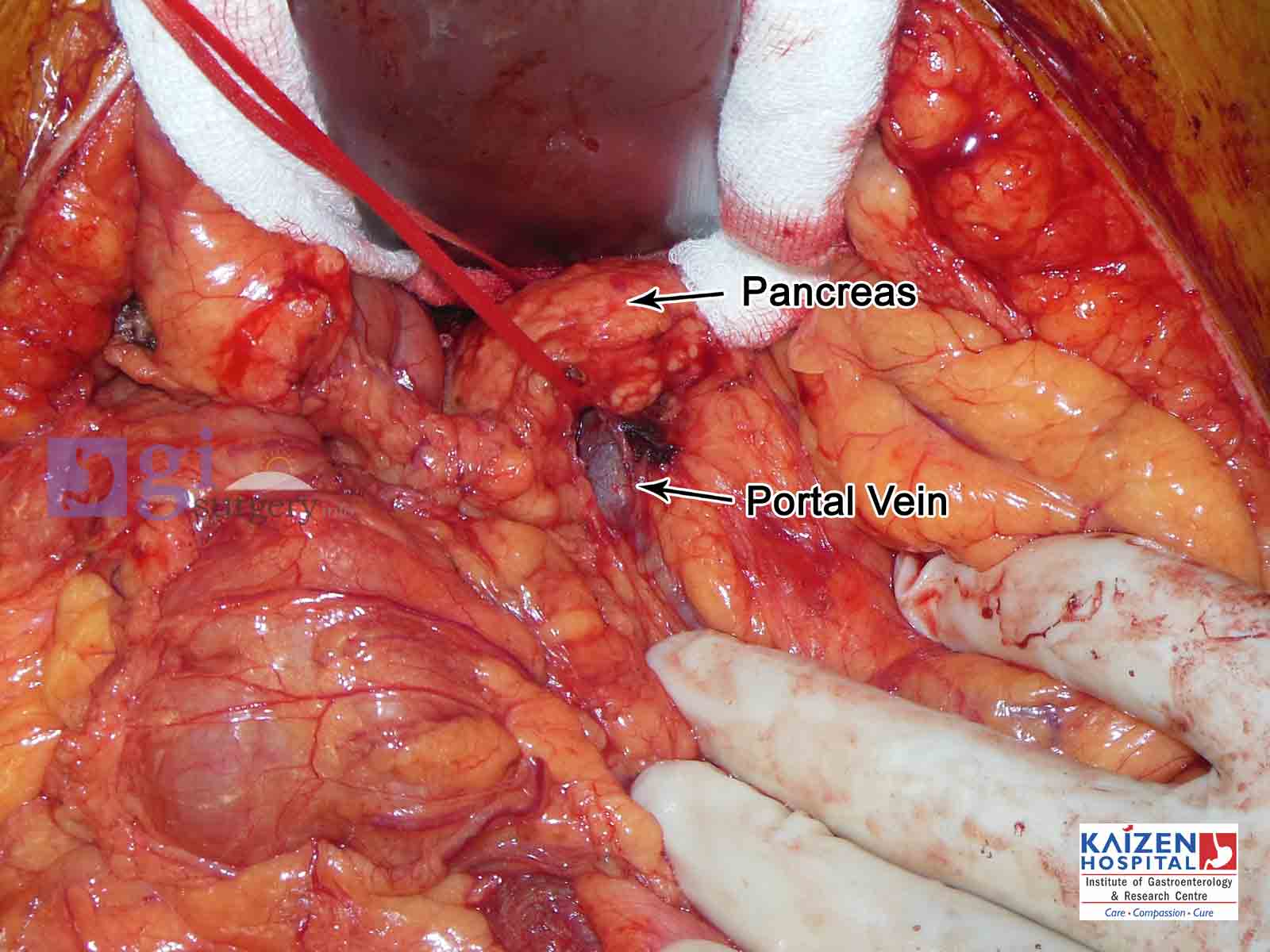
| Whipple's operation |
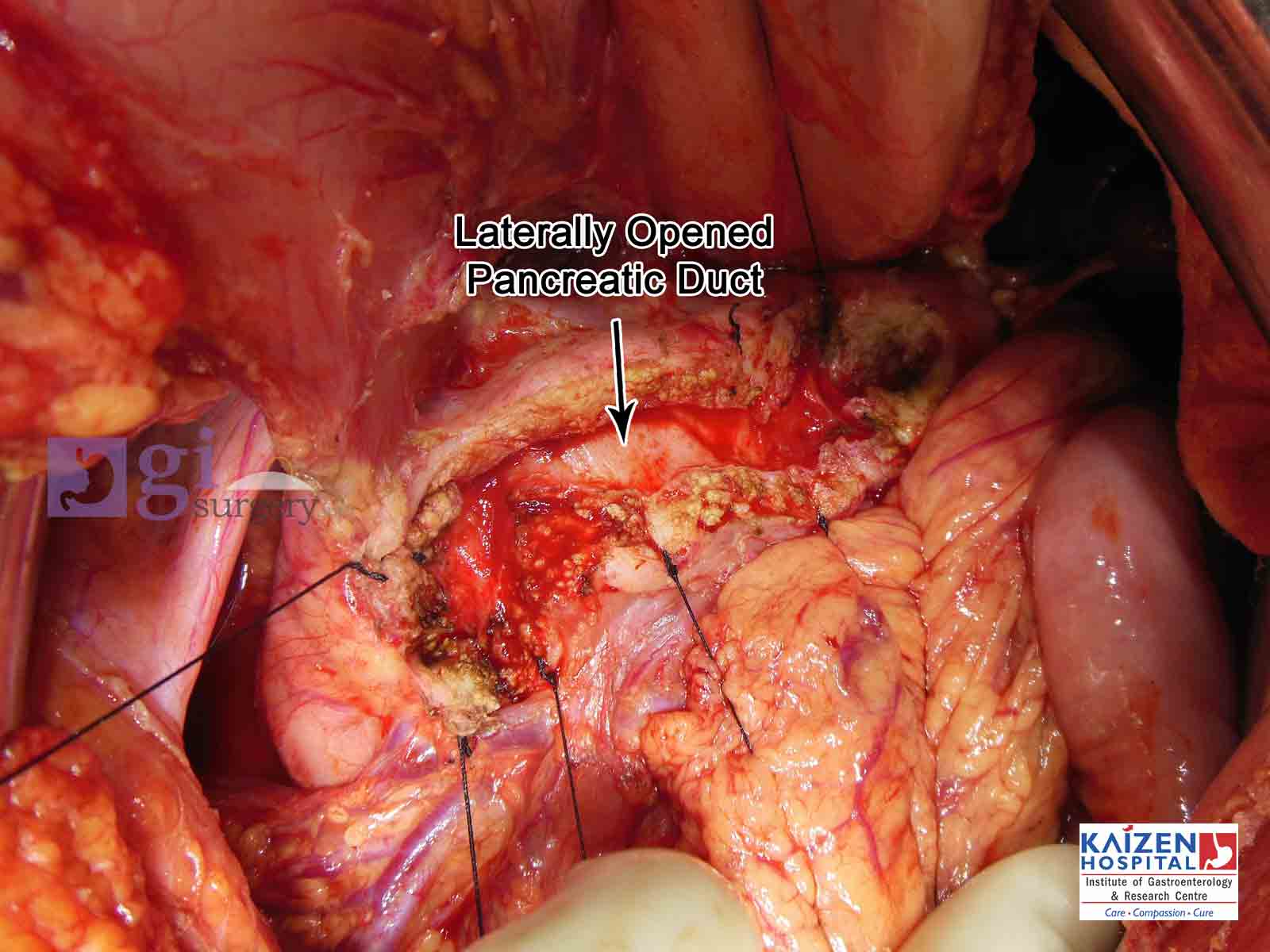
| Opened pancreatic duct |
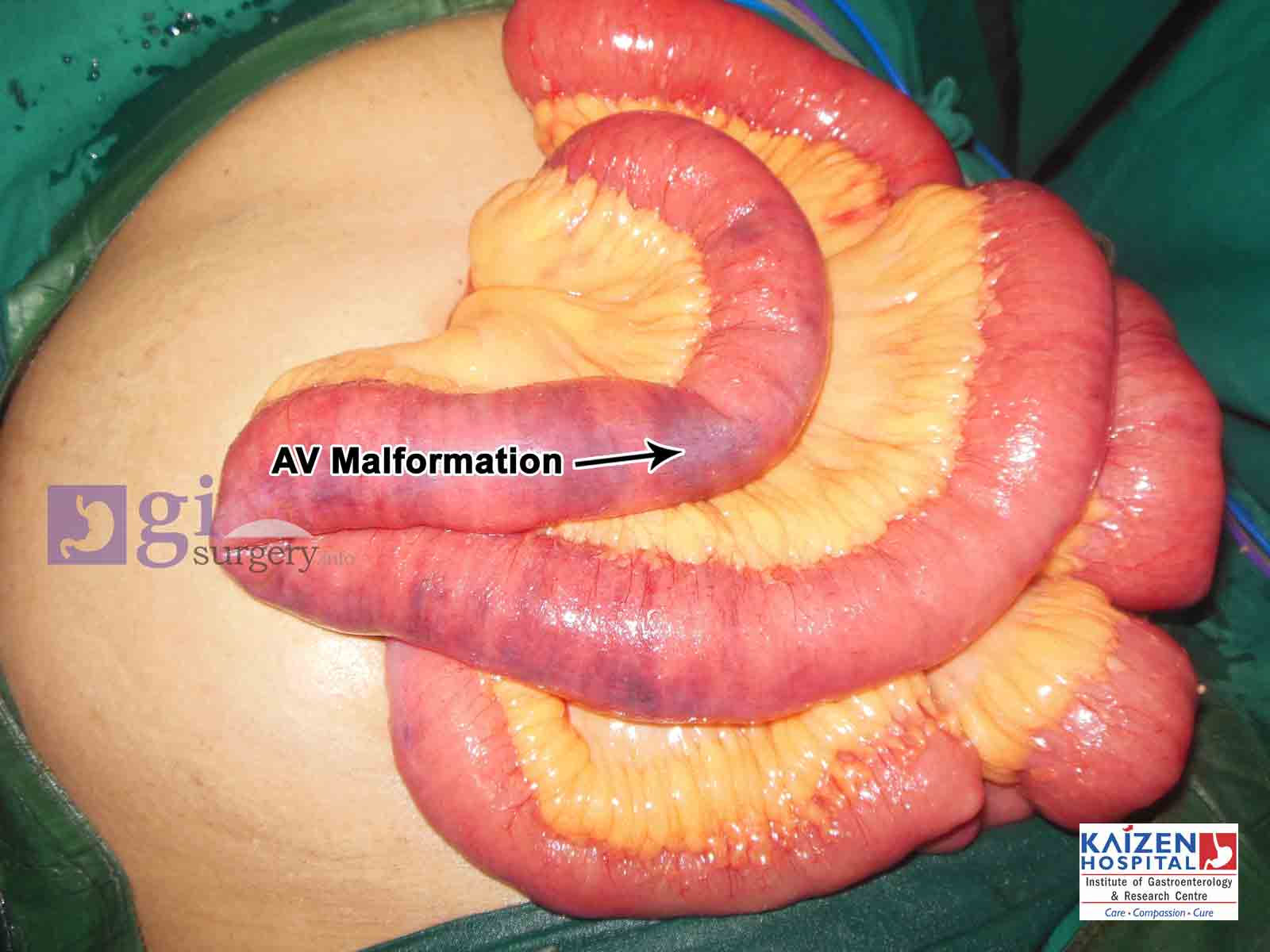
| AV Malformation of small intestine |
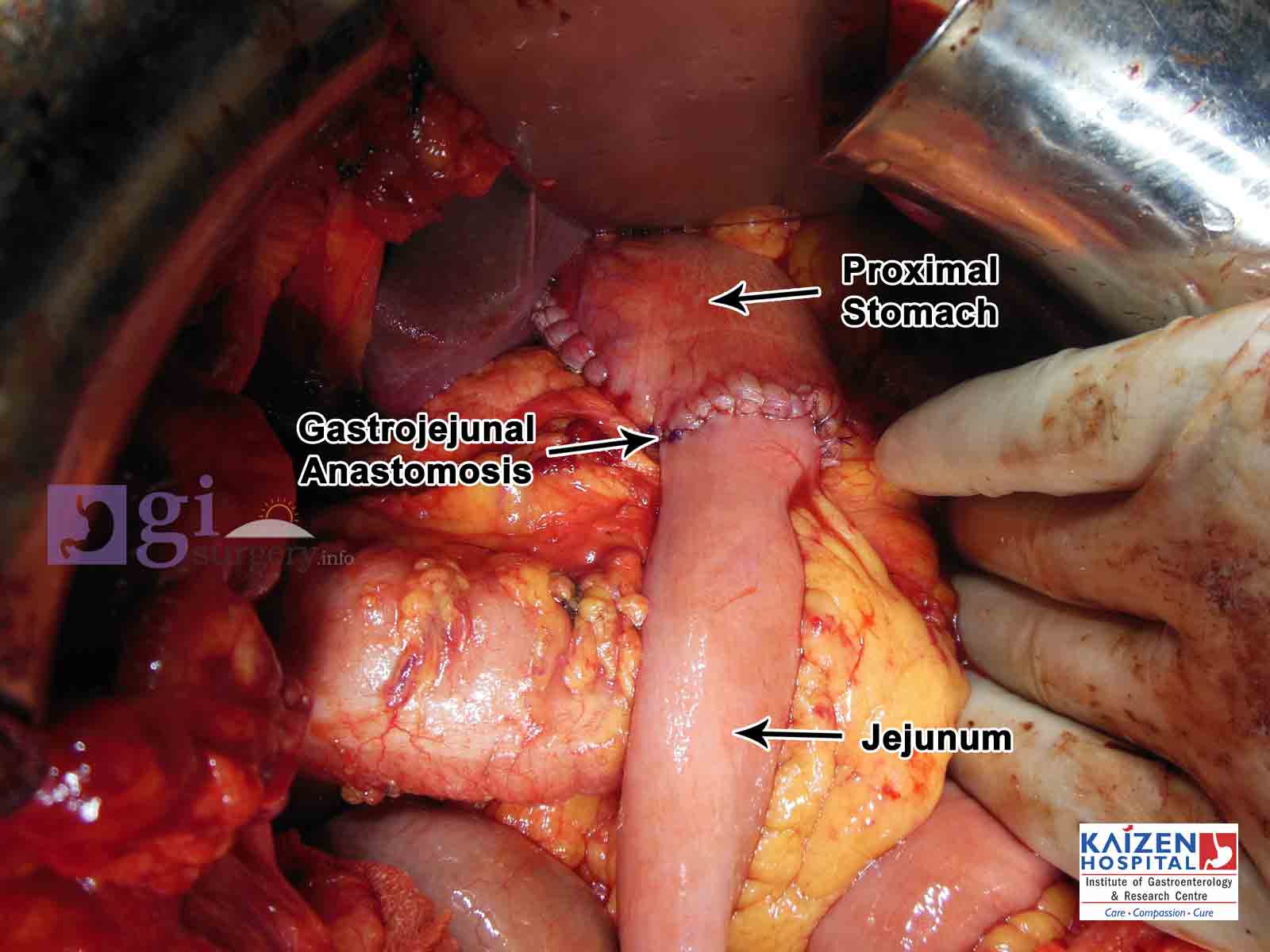
| Ca Stomach and patial gastrectomy |
| GIST tumour |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}