-

Haemetemesis and biliary leak after Lap Cholecystectomy
Dr. Sanjiv Haribhakti ( ), Kaizen HospitalMore- 58 year male presenting with c/o haemetemesis since 2 days.
- H/O Laparoscopic Cholecystectomy (elsewhere) 1 month ago.
- After 5 to 6 days of surgery, he had complain of abdominal pain which was treated conservatively elsewhere, as biliary pancreatitis.
- ERCP showed 2 leaks from cystic duct and stenting was done.
-

Diaphragmatic Hernia masquerading as Gastric volvulus
Dr. Sanjiv Haribhakti ( KAIZEN Hospital ), KAIZEN HospitalClinical HistoryMore- 32 years male presenting with c/o severe vomiting since 2 months.
- P/A - Upper abdominal fullness. Succussion splash.
-

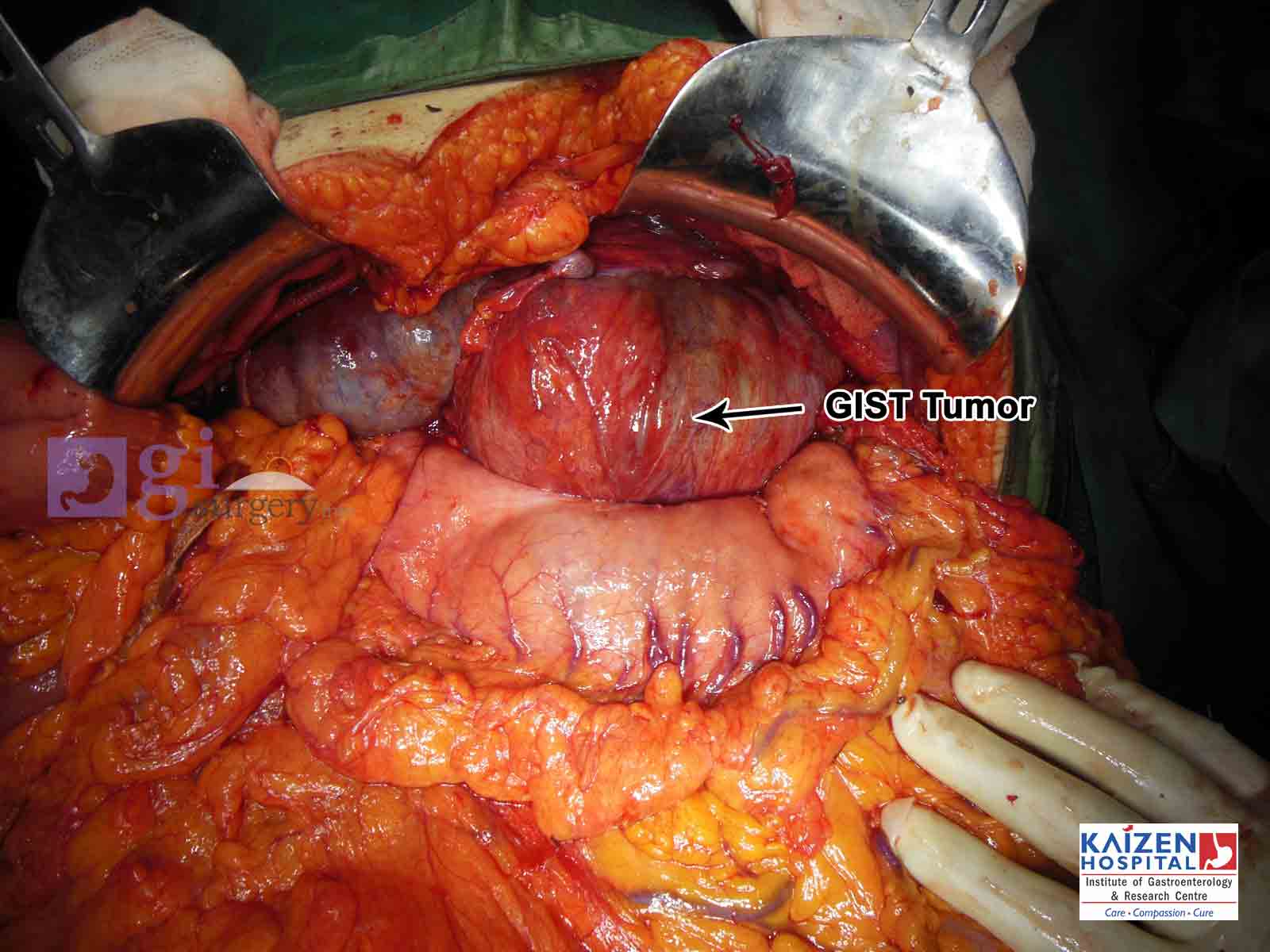
RECURRENT GIST (GASTRO-INTESTINAL STROMAL TUMOUR)
Dr. Sanjiv Haribhakti ( KAIZEN Hospital ), KAIZEN HospitalClinical HistoryMore- 34 years female presenting with c/o mild intermittent right hypochondriac and supra umbilical throbbing pain, epigastric and stomach burning, anorexia, generalised weakness since 3 months.
- H/O Laparotomy for duodenal mass (low grade GIST) – 7 years ago.
- P/A- Right paramedian small scar. No hernia. No mass palpable.
-

VARD (Video-assisted Retroperitoneal Debridement)
Dr. Sanjiv Haribhakti ( ), KAIZEN HospitalClinical History : 40 years male H/O blunt abdominal trauma. Left flank pain, fever off and on since 1 month. H/O Laparotomy.More -
 Dr. Sanjiv Haribhakti ( ), KAIZEN HospitalClinical History : 69 years anaemic (Hb- 5.5) male presenting with c/o generalised weakness since 20 days. K/c/o IHD- Triple Vessel Disease, HTN, DM. Colonoscopy was suggestive of descending colon mass with upper and distal rectal polyps.More
Dr. Sanjiv Haribhakti ( ), KAIZEN HospitalClinical History : 69 years anaemic (Hb- 5.5) male presenting with c/o generalised weakness since 20 days. K/c/o IHD- Triple Vessel Disease, HTN, DM. Colonoscopy was suggestive of descending colon mass with upper and distal rectal polyps.More -

Rare presentation of Intestinal Obstruction
Dr.Sanjiv Haribhakti ( ), KAIZEN HospitalClinical History :More- 73 years hypertensive, diabetic female presenting with c/o abdominal pain with distention, and nausea since 10 days.
- P/A- Distended abdomen with diffuse tenderness.
-

Endoscopic Excision of Large Gastric Polyp
Dr sanjiv Haribhakti ( Dr Sanjiv Haribhakti ), Kaizen HospitalMore- Even large polyps of the size 3.5 cm in the stomach can be removed endoscopically.
- The risk of bleeding can be minimised by applying an endoloop before doing the polypectomy.
- A surgical stand by should be ready while attempting endoscopic removal of large polyps.
-
_with_Mesh_gisurgery.info.jpg)
Component separation technique for a very large abdominal wall hernia
Dr Sanjiv Haribhakti ( ), Kaizen HospitalComponent separation technique for a very large abdominal wall herniaMore- 28 years male.
- Abdominal distention since 1 month.
- P/A- Large Ventral Hernia with widely gapping recti muscles, thinning of overlying skin, gross abdominal distention.
- Past history: Ileostomy and Colostomy for megacolon with Crohn’s Colitis followed by closure of stoma.
-

Conservative management of a rare complication of extensive small bowel haemorrhage
Dr Sanjiv Haribhakti ( ), Kaizen HospitalConservative management of a rare complication of extensive small bowel haemorrhage in a patient with cardiac valve replacement presenting as acute abdomenMore -

Colonic perforation in Ehlers Danlos Syndrome
Dr Sanjiv Haribhakti ( ), Kaizen HospitalMore- 49 yrs female, presented with abdominal distension with pain, nausea, vomiting, high grade fever since 4 days
- On Abdominal examination – abdomen was distended, diffuse tenderness all over, guarding, bowel sounds absent
- Known case of Ehlers Danlos Syndrome since childhood with typical features described later
view all
| Photos |
|---|
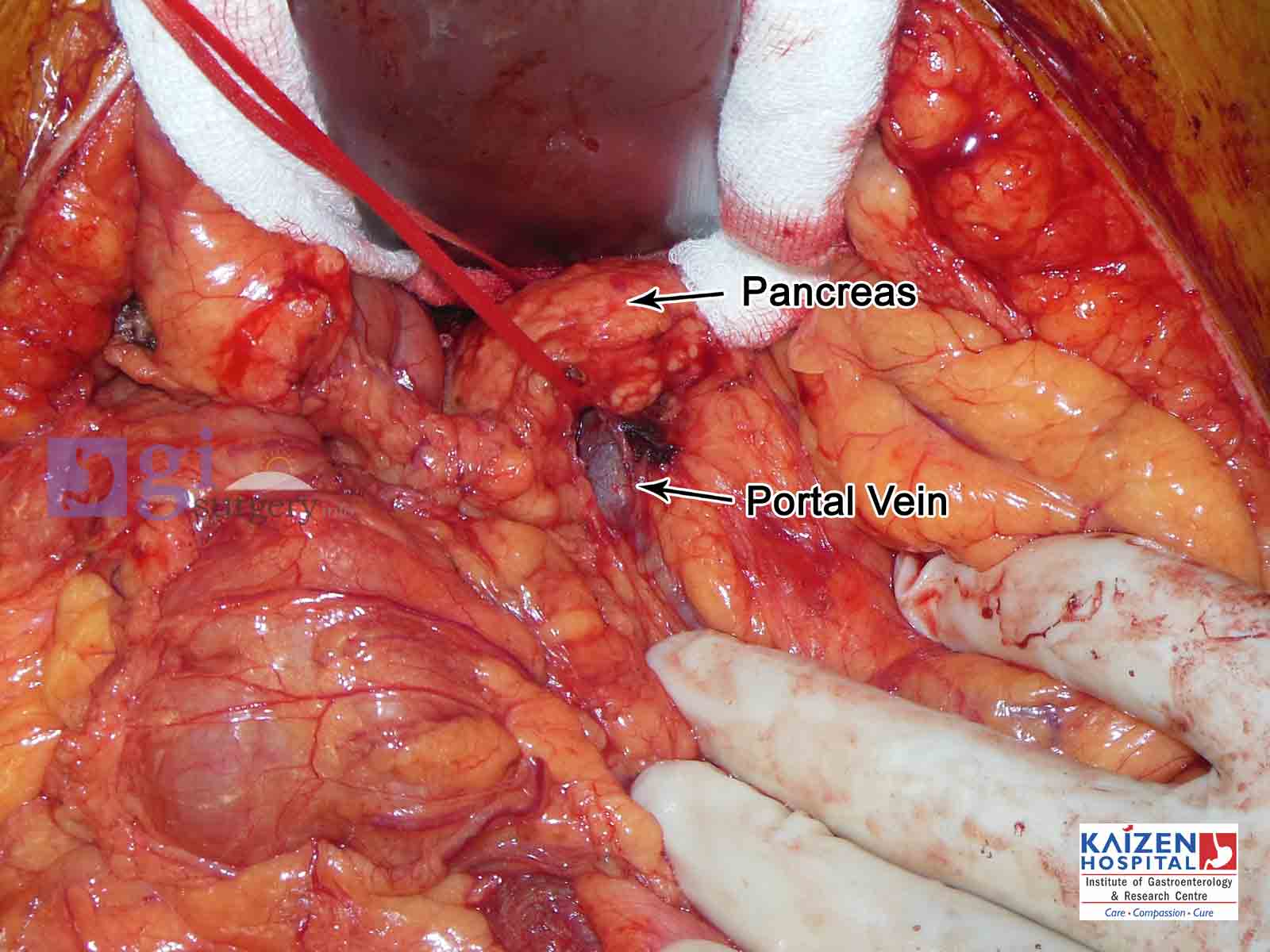
| Whipple's operation |
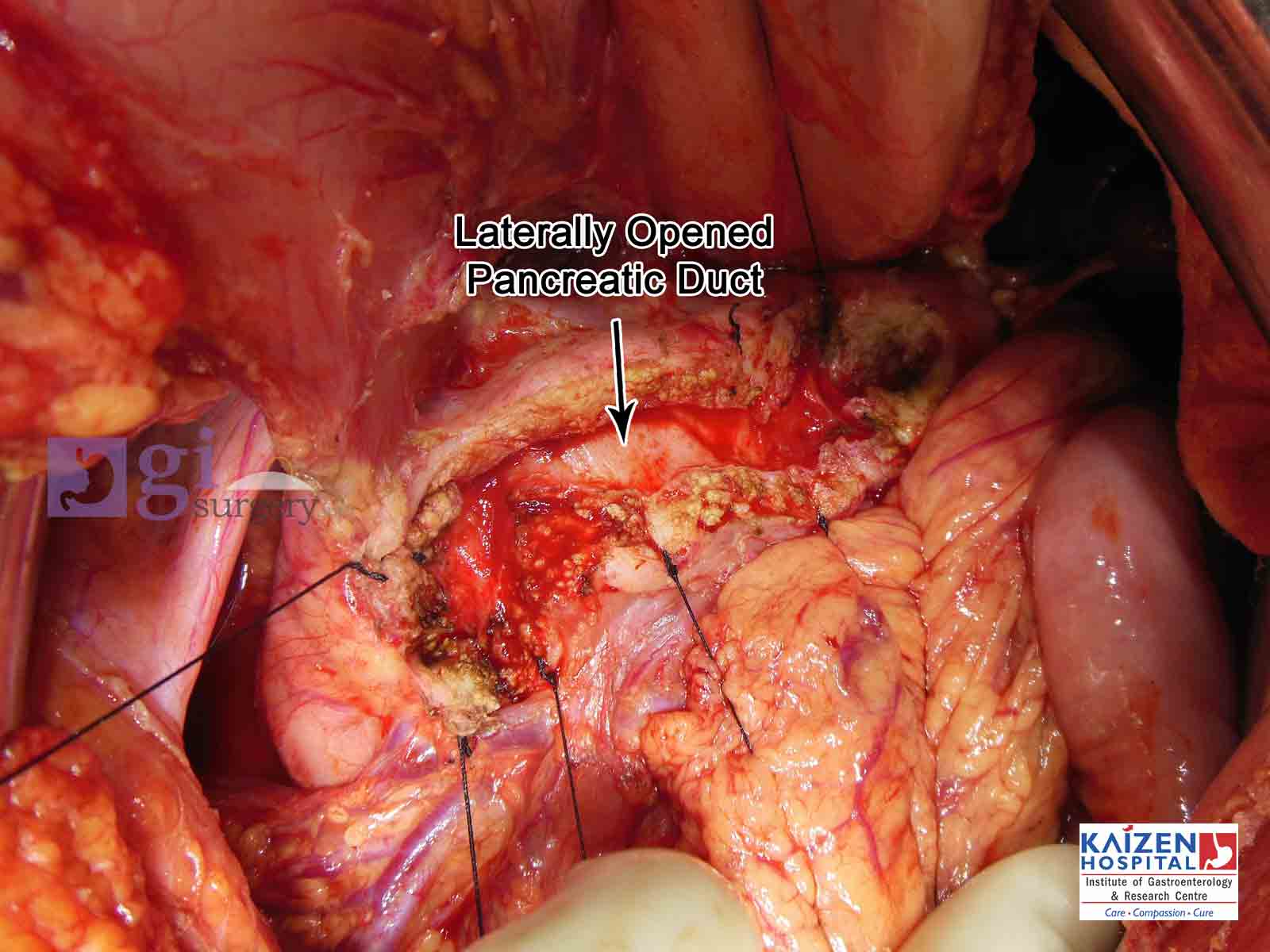
| Opened pancreatic duct |
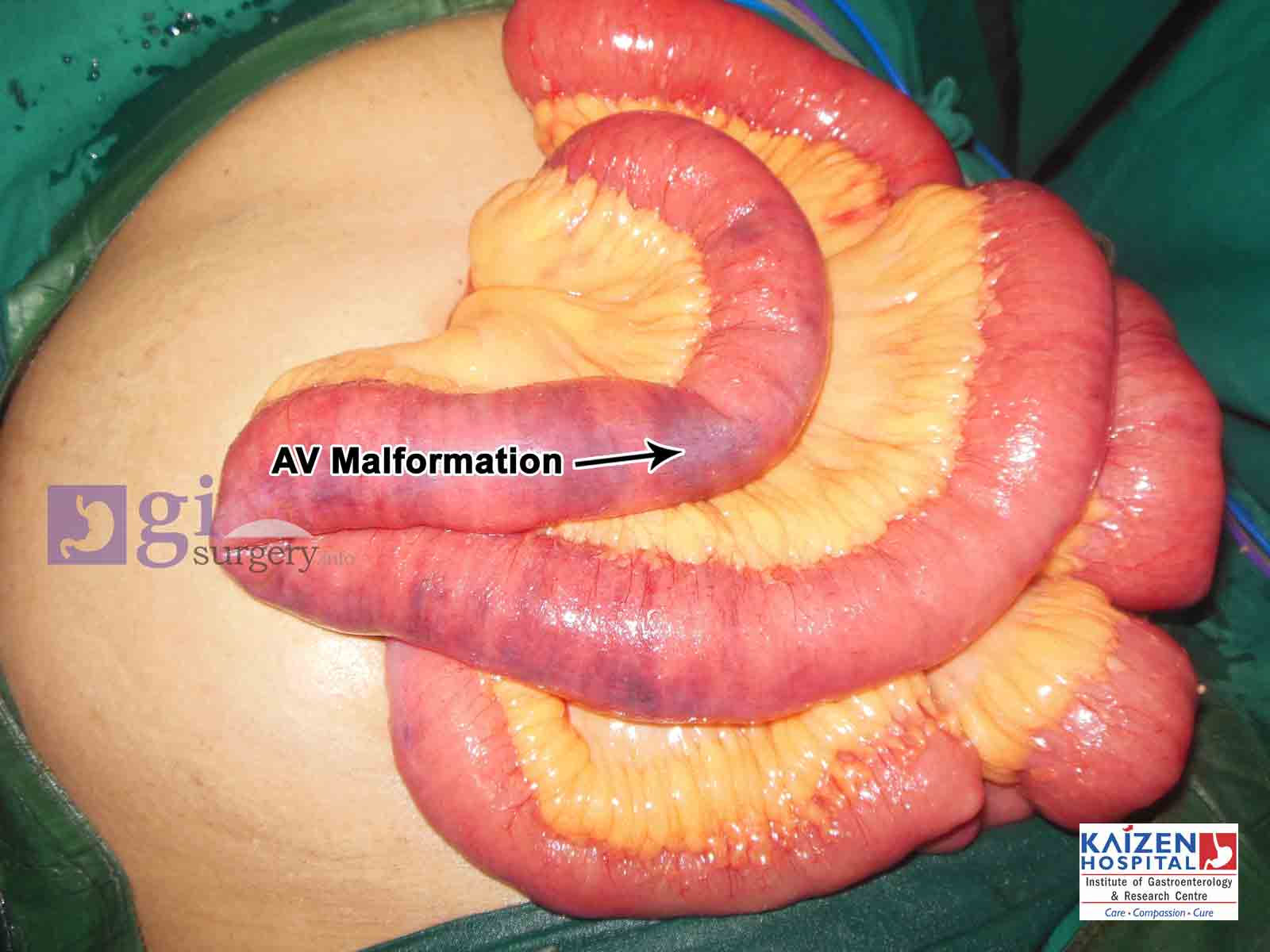
| AV Malformation of small intestine |
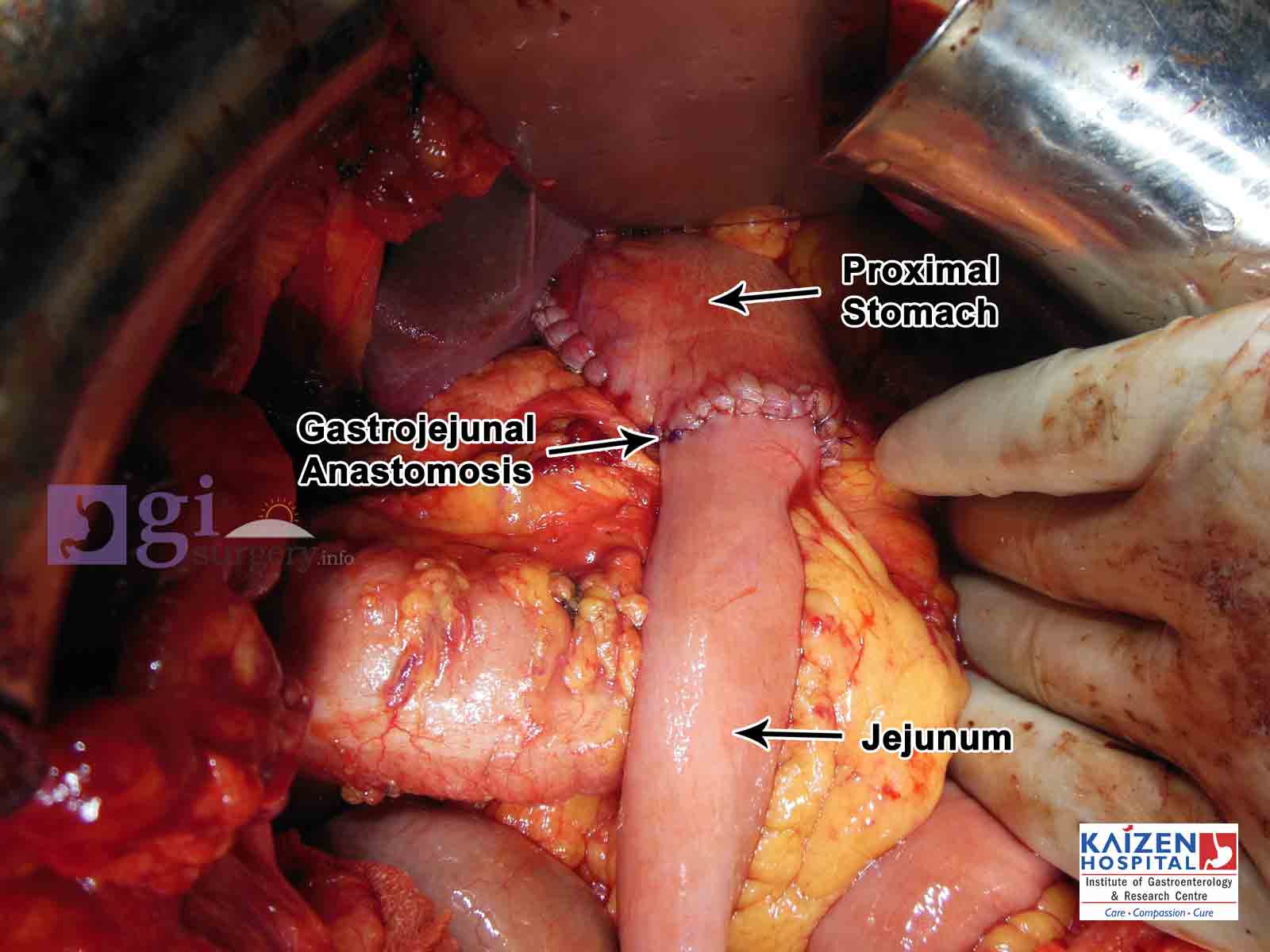
| Ca Stomach and patial gastrectomy |
| GIST tumour |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
view all
view all