New Treatments for Diabetic Gastroparesis Offer Promise
by Caroline Helwick
New treatments for diabetic gastroparesis appeared encouraging in two recent Phase II studies. One agent is still under development; the other is a novel formulation of the only FDA-approved product on the market for the condition, symptoms of which may, at some point, affect as many as half of patients with types 1 and 2 diabetes.
At the late-breaking abstract session at the 2014 Digestive Disease Week (DDW), investigators reported that a 10-mcg twice-daily subcutaneous dose of RM-131 significantly accelerated gastric emptying (GE) and led to clinically meaningful reductions in vomiting.
RM-131, also known as relamorelin (Rhythm Pharmaceuticals), is a selective ghrelin pentapeptide agonist under fast-track review by the FDA. RM-131 increases GE in patients with diabetes and is believed to be 15 to 130 times more potent than ghrelin, a gastric hormone that stimulates gastrointestinal activity.
“RM-131 met the study’s primary end point for gastric emptying, as well as key secondary end points,” said Anthony Lembo, MD, of Beth Israel Deaconess Medical Center, in Boston, who reported the findings.
Emptying improved by an average of 23 minutes from baseline after four weeks of twice-daily subcutaneous injections at the 10-mcg dose, Dr. Lembo reported.
The randomized, double-blind, placebo-controlled 28-day study (abstract 929a) involved 204 patients with a mean body mass index (BMI) of 33 kg/m2 , a Gastroparesis Cardinal Symptom Index (GCSI) of at least 2.6, and a history of nausea and/or vomiting at least once a week. Approximately 12% of patients had type 1 diabetes.
The screening GE breath test was performed at baseline and day 28 of the study. Symptoms were recorded daily, and the researchers analyzed a composite of nausea, abdominal pain, bloating and early satiety.
After a one-week run-in phase, patients were randomized to placebo before breakfast and before the evening meal; placebo before breakfast and RM-131 before the evening meal (i.e., RM-131 10-mcg once daily) or RM-131 before both meals (i.e., RM-131 10-mcg twice daily).
Changes in the placebo arm were significantly less than those observed in the active treatment group. The primary end point was change from baseline in GE breath test half-emptying time, which indirectly measures GE by determining concentrations of 13C-octanoid acid. In the modified intention-to-treat population (who received at least one dose), the change from baseline was –22.9 minutes with 10 mcg twice daily (P<0.001) and –7.5 with placebo, an absolute difference between the arms of 15.4 minutes.
In the 10-mcg once-daily group, the change from baseline was much less, –5.9 minutes, an insignificant difference over baseline measurement.
Twice-daily treatment also reduced weekly vomiting episodes by 63% (P=0.033) and vomiting severity by 58% (P=0.005) compared with placebo.
A strong placebo effect was present for symptoms of nausea, abdominal pain, bloating and early satiety, and in the composite end point. “The effects of RM-131 were numerically greater, but not significantly different from placebo,” Dr. Lembo said.
Most Benefit Seen in Vomiting Subgroup
Approximately 60% of the study population reported vomiting at baseline, with a mean of five to six episodes per week. RM-131 had a significant effect in this subgroup of 119 patients, reducing mean GE breath test by 30.6 minutes over baseline, and vomiting episodes by 63%.
“We did this subgroup [post hoc] analysis because vomiting is the most bothersome symptom and often brings the patient in for treatment,” Dr. Lembo said. In contrast to the overall population, for the four subjective patient-reported symptoms, “a clear separation from placebo was demonstrated,” Dr. Lembo reported.
The composite score separated from placebo within one week, and was statistically significant at weeks 2, 3 and 4 of the study. Overall, there were no safety concerns with the drug, which had no effect on weight, Dr. Lembo said. Adverse events were reported by 43% of the placebo group, 48% of the once-daily treatment arm and 37% of the twice-daily group.
Pankaj Jay Pasricha, MD, professor of medicine at Johns Hopkins University and director of the Johns Hopkins Center for Motility Disorders and Digestive Diseases, in Baltimore, said, “There are few drugs with positive results in diabetic gastroparesis, and I hope this one moves forward.”
Metoclopramide Nasal Spray
Metoclopramide is the only FDA-approved drug for treating symptoms of gastroparesis. A nasal spray formulation (EVK-110) is being developed to provide reliable systemic absorption, even when patients are experiencing a disease flare. Systemic concentrations are about 85% of the orally administered dose.
“A prior head-to-head study suggested the nasal spray has advantages over an orally administered tablet, including better symptom control in diabetic patients with gastroparesis,” said Henry P. Parkman, MD, director of the GI Motility Laboratory at Temple University School of Medicine, in Philadelphia, who presented Phase IIb results at DDW (abstract 71).
“This Phase IIb study was the largest clinical study in diabetic gastroparesis with metoclopramide. The results were encouraging and quite unexpected,” Dr. Parkman said. “Metoclopramide nasal spray provided a significant clinical benefit in reducing the symptoms of diabetic gastroparesis in women, whereas in men it did not.”
More than 80% of patients with diabetic gastroparesis are women, Dr. Parkman noted, so the latest findings are “important new information. Metoclopramide nasal spray has the potential to address an unmet need for patients.”
The multicenter, double-blind, placebo-controlled trial compared two doses (10 and 14 mg) of metoclopramide nasal spray in 287 patients with symptomatic diabetic gastroparesis (mean age 51; 71% women). The primary end point was change from baseline to week 4 in the modified daily dietary version of the GCSI total score (nausea, early satiety, bloating and upper abdominal pain).
“Overall, the primary efficacy end point was not statistically significant,” Dr. Parkman said (Table). “This appeared to be due to the high placebo response, primarily in male patients. Females, but not males, had statistically significant improvement in symptoms for both doses of intranasal metoclopramide.”
toclopramide.”
|
||||||||||||||||||||||||||||||||||||
For the primary end point, an interaction test between treatment and sex was statistically significant (P=0.038), suggesting the effect of the drug differs between men and women, he said. “The observed differences in efficacy by gender were not related to severity of baseline disease or other demographic characteristics,” he added.
Dr. Parkman said the patients tolerated the nasal spray well at both doses. “There were no dose-limiting toxicities and fewer than 10% of patients dropped out, including 5% due to adverse events,” he said.
The majority of adverse events were mild or moderate, and there were no deaths or reports of tardive dyskinesia, he added.
“These two studies offer potentially very exciting new options for the treatment of a very common problem for a large number of diabetic patients,” said David A. Johnson, MD, professor of medicine and chief of gastroenterology at Eastern Virginia Medical School, in Norfolk. He said the lack of tardive dyskinesia and tremor with the metoclopramide nasal spray is notable.
“Improving gastric emptying in these patients is important for both symptom relief as well as glycemic control,” Dr. Johnson said. “At present, we have very limited effective options for these patients, and these data address a huge unmet therapeutic need.”
New Treatments for Diabetic Gastroparesis Offer Promise
by Caroline Helwick
New treatments for diabetic gastroparesis appeared encouraging in two recent Phase II studies. One agent is still under development; the other is a novel formulation of the only FDA-approved product on the market for the condition, symptoms of which may, at some point, affect as many as half of patients with types 1 and 2 diabetes.
At the late-breaking abstract session at the 2014 Digestive Disease Week (DDW), investigators reported that a 10-mcg twice-daily subcutaneous dose of RM-131 significantly accelerated gastric emptying (GE) and led to clinically meaningful reductions in vomiting.
RM-131, also known as relamorelin (Rhythm Pharmaceuticals), is a selective ghrelin pentapeptide agonist under fast-track review by the FDA. RM-131 increases GE in patients with diabetes and is believed to be 15 to 130 times more potent than ghrelin, a gastric hormone that stimulates gastrointestinal activity.
“RM-131 met the study’s primary end point for gastric emptying, as well as key secondary end points,” said Anthony Lembo, MD, of Beth Israel Deaconess Medical Center, in Boston, who reported the findings.
Emptying improved by an average of 23 minutes from baseline after four weeks of twice-daily subcutaneous injections at the 10-mcg dose, Dr. Lembo reported.
The randomized, double-blind, placebo-controlled 28-day study (abstract 929a) involved 204 patients with a mean body mass index (BMI) of 33 kg/m2 , a Gastroparesis Cardinal Symptom Index (GCSI) of at least 2.6, and a history of nausea and/or vomiting at least once a week. Approximately 12% of patients had type 1 diabetes.
The screening GE breath test was performed at baseline and day 28 of the study. Symptoms were recorded daily, and the researchers analyzed a composite of nausea, abdominal pain, bloating and early satiety.
After a one-week run-in phase, patients were randomized to placebo before breakfast and before the evening meal; placebo before breakfast and RM-131 before the evening meal (i.e., RM-131 10-mcg once daily) or RM-131 before both meals (i.e., RM-131 10-mcg twice daily).
Changes in the placebo arm were significantly less than those observed in the active treatment group. The primary end point was change from baseline in GE breath test half-emptying time, which indirectly measures GE by determining concentrations of 13C-octanoid acid. In the modified intention-to-treat population (who received at least one dose), the change from baseline was –22.9 minutes with 10 mcg twice daily (P<0.001) and –7.5 with placebo, an absolute difference between the arms of 15.4 minutes.
In the 10-mcg once-daily group, the change from baseline was much less, –5.9 minutes, an insignificant difference over baseline measurement.
Twice-daily treatment also reduced weekly vomiting episodes by 63% (P=0.033) and vomiting severity by 58% (P=0.005) compared with placebo.
A strong placebo effect was present for symptoms of nausea, abdominal pain, bloating and early satiety, and in the composite end point. “The effects of RM-131 were numerically greater, but not significantly different from placebo,” Dr. Lembo said.
Most Benefit Seen in Vomiting Subgroup
Approximately 60% of the study population reported vomiting at baseline, with a mean of five to six episodes per week. RM-131 had a significant effect in this subgroup of 119 patients, reducing mean GE breath test by 30.6 minutes over baseline, and vomiting episodes by 63%.
“We did this subgroup [post hoc] analysis because vomiting is the most bothersome symptom and often brings the patient in for treatment,” Dr. Lembo said. In contrast to the overall population, for the four subjective patient-reported symptoms, “a clear separation from placebo was demonstrated,” Dr. Lembo reported.
The composite score separated from placebo within one week, and was statistically significant at weeks 2, 3 and 4 of the study. Overall, there were no safety concerns with the drug, which had no effect on weight, Dr. Lembo said. Adverse events were reported by 43% of the placebo group, 48% of the once-daily treatment arm and 37% of the twice-daily group.
Pankaj Jay Pasricha, MD, professor of medicine at Johns Hopkins University and director of the Johns Hopkins Center for Motility Disorders and Digestive Diseases, in Baltimore, said, “There are few drugs with positive results in diabetic gastroparesis, and I hope this one moves forward.”
Metoclopramide Nasal Spray
Metoclopramide is the only FDA-approved drug for treating symptoms of gastroparesis. A nasal spray formulation (EVK-110) is being developed to provide reliable systemic absorption, even when patients are experiencing a disease flare. Systemic concentrations are about 85% of the orally administered dose.
“A prior head-to-head study suggested the nasal spray has advantages over an orally administered tablet, including better symptom control in diabetic patients with gastroparesis,” said Henry P. Parkman, MD, director of the GI Motility Laboratory at Temple University School of Medicine, in Philadelphia, who presented Phase IIb results at DDW (abstract 71).
“This Phase IIb study was the largest clinical study in diabetic gastroparesis with metoclopramide. The results were encouraging and quite unexpected,” Dr. Parkman said. “Metoclopramide nasal spray provided a significant clinical benefit in reducing the symptoms of diabetic gastroparesis in women, whereas in men it did not.”
More than 80% of patients with diabetic gastroparesis are women, Dr. Parkman noted, so the latest findings are “important new information. Metoclopramide nasal spray has the potential to address an unmet need for patients.”
The multicenter, double-blind, placebo-controlled trial compared two doses (10 and 14 mg) of metoclopramide nasal spray in 287 patients with symptomatic diabetic gastroparesis (mean age 51; 71% women). The primary end point was change from baseline to week 4 in the modified daily dietary version of the GCSI total score (nausea, early satiety, bloating and upper abdominal pain).
“Overall, the primary efficacy end point was not statistically significant,” Dr. Parkman said (Table). “This appeared to be due to the high placebo response, primarily in male patients. Females, but not males, had statistically significant improvement in symptoms for both doses of intranasal metoclopramide.”
toclopramide.”
|
||||||||||||||||||||||||||||||||||||
For the primary end point, an interaction test between treatment and sex was statistically significant (P=0.038), suggesting the effect of the drug differs between men and women, he said. “The observed differences in efficacy by gender were not related to severity of baseline disease or other demographic characteristics,” he added.
Dr. Parkman said the patients tolerated the nasal spray well at both doses. “There were no dose-limiting toxicities and fewer than 10% of patients dropped out, including 5% due to adverse events,” he said.
The majority of adverse events were mild or moderate, and there were no deaths or reports of tardive dyskinesia, he added.
“These two studies offer potentially very exciting new options for the treatment of a very common problem for a large number of diabetic patients,” said David A. Johnson, MD, professor of medicine and chief of gastroenterology at Eastern Virginia Medical School, in Norfolk. He said the lack of tardive dyskinesia and tremor with the metoclopramide nasal spray is notable.
“Improving gastric emptying in these patients is important for both symptom relief as well as glycemic control,” Dr. Johnson said. “At present, we have very limited effective options for these patients, and these data address a huge unmet therapeutic need.”
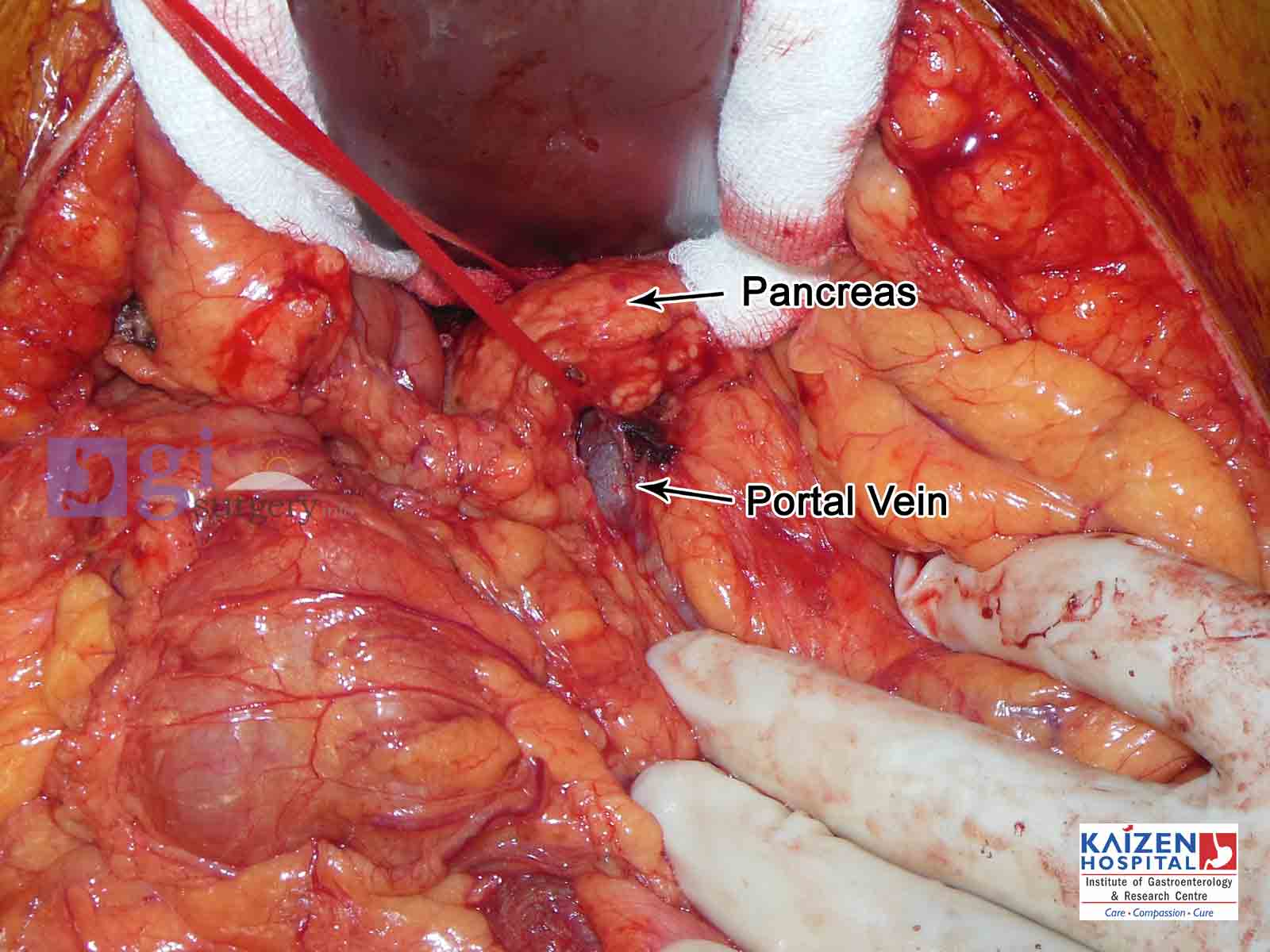
| Photos |
|---|
| Whipple's operation |
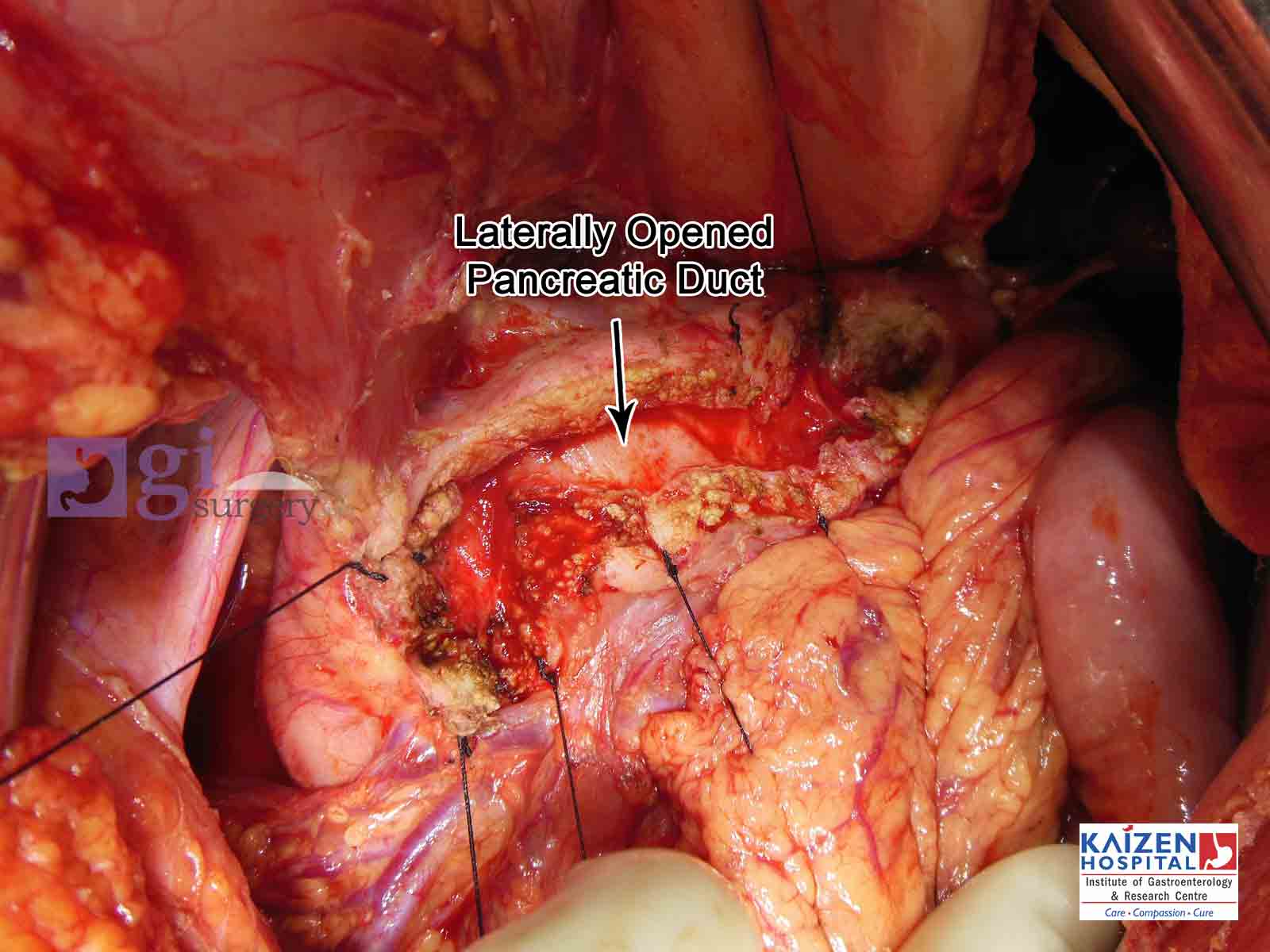
| Opened pancreatic duct |
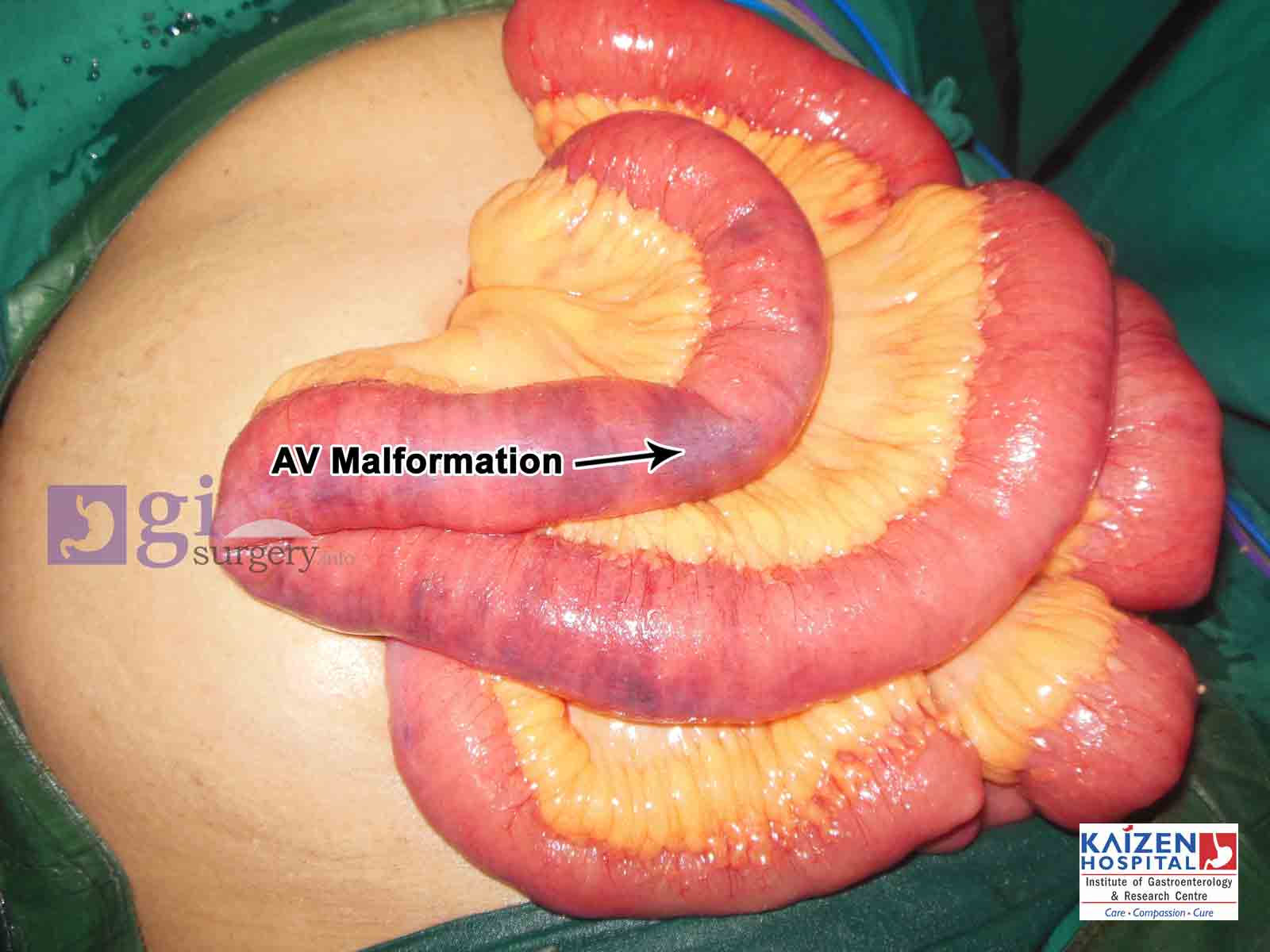
| AV Malformation of small intestine |
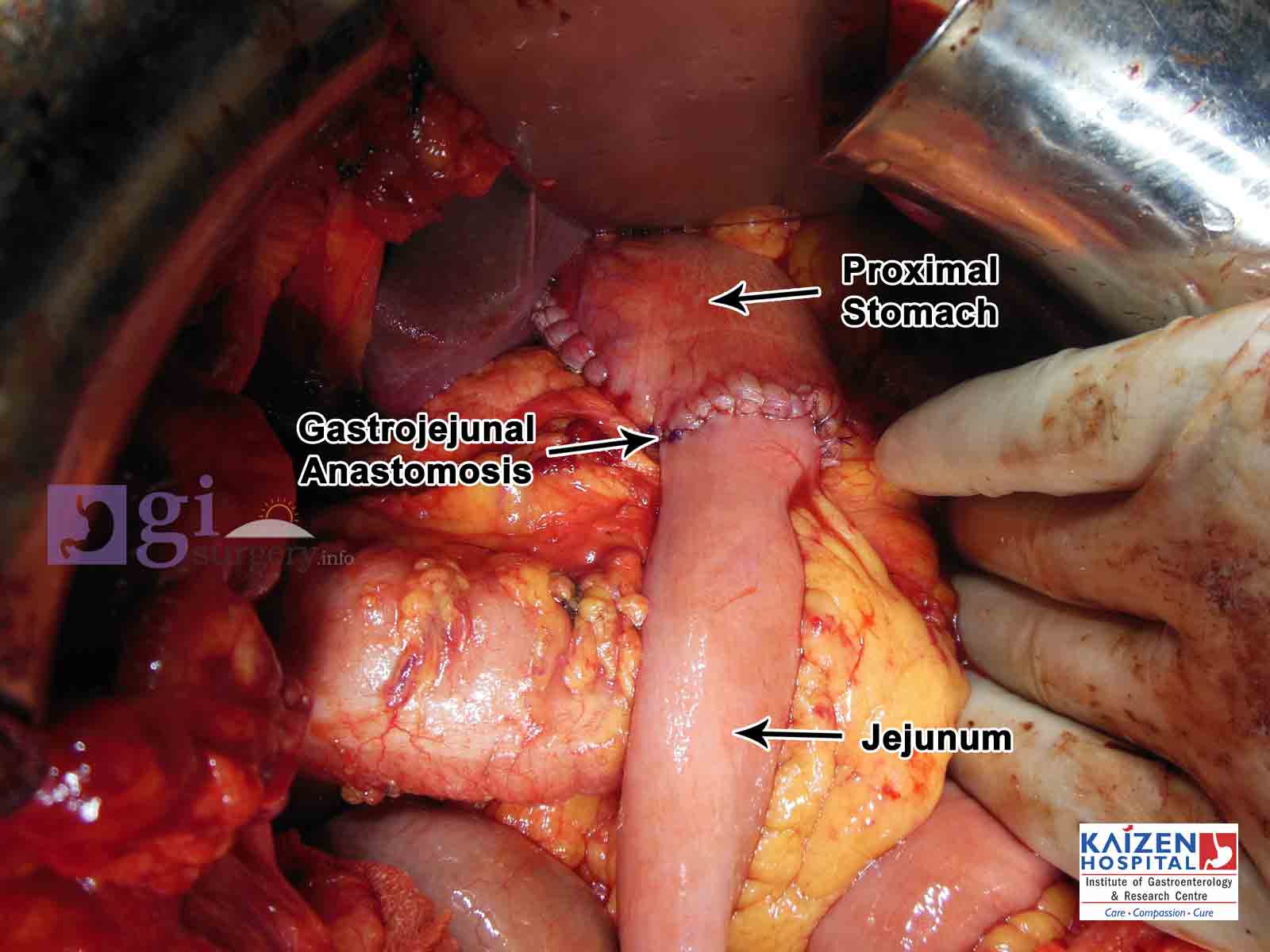
| Ca Stomach and patial gastrectomy |
| GIST tumour |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}